Just following on from the feedback from my last post about process v outcome in safety management, below if a short video I did a little while ago that explains some of the concepts further.
Enjoy.
Just following on from the feedback from my last post about process v outcome in safety management, below if a short video I did a little while ago that explains some of the concepts further.
Enjoy.
Today I was reading a LinkedIn post lamenting the state of health and safety management, evidenced by too many “safety stickers” on a piece of machinery.
A commenter noted that the situation was “absolute madness“, which doesn’t keep anyone safe. Much of the conversation from there was focused on whose “fault” it was and we ended up with all of the usual suspects in the firing line – insurers, lawyers, consultants and so on. Probably quite justified too.
To my mind, this issue illustrates the disconnect apparent in health and safety management between “process” and “outcome“. It seems to me that health and safety management is obsessed with process – the way that we “do” safety. This obsession means that every few years somebody reinvents the way we do safety, or the way we do parts of safety. As evidence of this you only need to think of the transition from safety culture, to safety 1, through to safety 2 and now safety differently – with god only knows what in between. On a micro level, just think how many iterations of the JHA you have seen during your working career.
What makes this more interesting is the process doesn’t really matter. How you “do” safety is not really an issue. What is important is whether you can show your process achieves the outcome it was designed for.
The table below lists a series of cases looking at the “outcome” of understanding hazards. The “processes” were all different: documented, undocumented, buddy systems, on-the-job training and so on. But even where the processes were the same this did not determine the decision – the decision was determined on whether the outcome, and understanding of hazards and risks, was achieved.
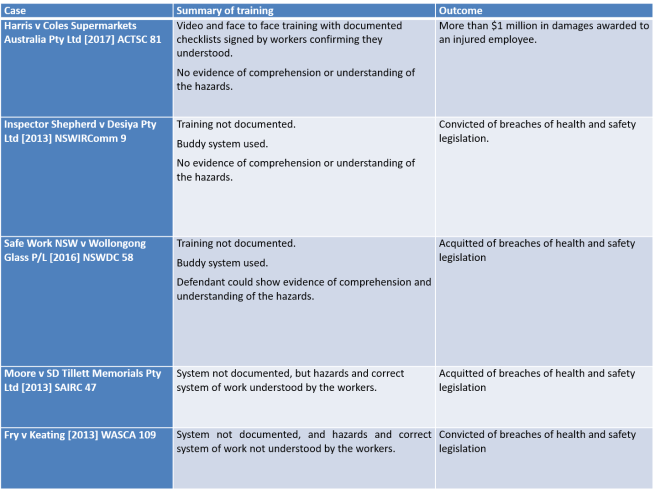
So, the question is not how fancy, new or shiny your process is. The question is whether it achieves the outcome.
When you survey the range of safety commentary online, it is hard to escape the view that workplace health and safety is still primarily concerned with the behaviour of individual workers, and incidents are the consequence of careless individuals.
In my experience, this thinking does not align with any credible safety management theory, and it is not consistent with an organisation’s obligations under health and safety legislation. At its simplest, a worker’s individual carelessness makes no difference to the obligations of their employer, other organisations or other individuals under health and safety legislation.
The fact that a careless, individual worker did not meet their obligations under health and safety legislation, is no answer to the question of whether you met yours.
In the recent NSW District Court decision, Inspector Nash v Perilya Broken Hill Limited [2018] NSWDC 28 (read decision) the Court canvassed the issue of careless and disobedient workers in detail.
By way of background, On 8 June 2012, an employee of Perilya Broken Hill Limited (PBHL), Mark Pollard suffered a traumatic amputation of his right leg and other injuries when he fell down a haulage shaft at a mine in Broken Hill (Mine). At the time of the incident Mr Pollard, was trying to hang some weights from the bottom of a weigh flask to calibrate an instrument a load cell which measured the weight of ore in the flask.
The weights were in a metal basket and the weight Mr Pollard was hanging was about 10 tonnes. The weights and basket were in the bucket of a loader. Mr Pollard was trying to hang the weights by working from the bucket of the loader, the bucket being located in the haulage shaft.
Mr Pollard was secured to the bucket by personal protective equipment (PPE), a fall arrest system comprising harness and lanyard. His lanyard was tied to the bucket.
While Mr Pollard was working, the weights and basket fell out of the bucket and so did Mr Pollard. His lanyard snapped, and he fell.
The Court said:
In view of the fact that the workers used the bucket of the loader contrary to the understood policy prohibiting it, it is appropriate to look at authorities involving cases of careless or disobedient workers.[my emphasis added]
Drawing on precedent cases, the Court made several observations:
The duty to provide a risk free work environment is a duty owed not only to the careful and observant employee but also to the hasty, careless, inadvertent, inattentive, unreasonable or disobedient employee in respect of conduct that is reasonably foreseeable…
It may be that, in some cases, it would not be practicable to guard against a detriment to safety occasioned by an appropriately trained and instructed employee departing from a known safe procedure. This may be so because the risk of the employee failing to follow procedures was not reasonably foreseeable or on a comparison of the training and instruction required to ensure the employee adhered to those procedures with the risks created. There are limits to the degree of instruction which can be expected to be provided to an experienced employee.
Where an employer is found to have laid down a safe and proper practice and there is no evidence that the employer failed to use due diligence to see that the practice is observed, then a casual failure by inferior employees, even if of supervisory rank, to observe that practice on a particular occasion will not render the employer criminally liable for a failure to ensure safety.
In the PBHL case, the Court rejected any argument that carelessness by individual workers limited PBHL’s liability:
I do not see any scope for the application of a principle in this case that would limit the defendant’s liability where the very risk that is in issue is one that was foreseen by Mr Dally and by Mr Slade, where Mr Dally told Messrs Tavian, Harris, Ridley and Gauci that he did not want the workers working the bucket of the loader and where he expected that to be passed on to the workers, and where he expected that to be in the JSA.
Mr Dally and Mr Slade both expected the JSA to cover the risk of the use of the bucket and/or falling from height and it did not. [my emphasis added]
The Court found procedures and instructions for the work were incomplete and workers were directed to start work when the JSA process was deficient and the JSA document was inadequate. The employer should have known both those things.
A common misconception is that safety prosecutions are all about identifying “fault” – who was at fault, or most at fault, when an accident occurred. This is not the case.
Employees who breach known safety procedures may be at “fault”. Indeed, individual workers and supervisors are prosecuted following workplace accidents. But an employees fault is no answer to the question, “did the employer meet their obligations under health and safety legislation?”.
The fact an employee breached safety procedures – even procedures they were aware of, does not prove an employer provided adequate training and supervision, nor does it prove an employer diligently enforced its systems of work.
This is a call out to all of my connections in New Zealand.
Dr Rob Long and I will be in New Zealand at the end of August, running due diligence programs for clients. While we are in Auckland, we want to take the opportunity to run some 1-day, public due diligence programs, and are calling for expressions of interest for either 30 or 31 August.
During the program we will be discussing ideas from our book, Risk Conversations: The Law, Social Phycology and Risk. You can also see our discussion about due diligence from the book, in the video below.
The expected cost of the 1-day program is $495 (AUD) plus GST.
You can access more information about the program HERE. You can also email me directly- gws@nexuslawyers.com.au – or email admin@humandymensions.com.
It seems hardly a day goes by without social media raising a new discussion about the merits or otherwise of “Zero Harm”.
As I understand the various arguments “for” and “against”, there seemed to be three broad categories of argument (although I do not discount further or additional arguments).
One argument says that Zero Harm is not a target, or a goal, rather it is an aspiration – something to pursue. If I may be so bold as to paraphrase Prof Andrew Hopkins, it is like a state of grace – something to be striven for, but never truly achieved.
Another argument, more of a middle ground, articulates that Zero Harm is “okay”, but may have an unintended consequence of driving adverse behaviour. In particular, it is argued that Zero Harm causes individuals and organisations to hide incidents or manipulate injury data in support of an organisation’s “zero” targets.
Yet another argument says that the language of zero is totally corrosive and destructive. It argues the language of zero – amongst other things – primes a discourse that is anti-learning and anti-community (See, For the Love of Zero by Dr Robert Long).
I would like to use this article to discuss two matters. First, the Safety Paradox in the context of aspirational statements, only using “zero” as a starting example. Second, to demonstrate how aspirational statements can be used against organisations. Both these points are closely related but ultimately, I want to argue whatever your “aspirations” you need to have “assurance” about the effect they have on your business.
The Safety Paradox is a concept I have been exploring for some time now. The Safety Paradox supposes that our safety initiatives have within them the potential to improve safety and cause harm.
In my view, the single biggest weakness in modern safety management is the assumption that safety management initiatives are “good“. I have no doubt that the proponents of Zero Harm suffer from this assumption.
The question of whether Zero Harm is good or bad is, on one view, totally irrelevant. If you are a Zero Harm organisation the only thing that really matters is the impact Zero Harm has in your workplace.
My personal experience with Zero Harm means that I remain unconvinced of its benefits, but I do not feel I am closed to being persuaded otherwise, it is just that I have never worked with an organisation that has been able to address the three questions proposed above. Moreover, in my experience, there is usually a significant disconnect between corporate intentions and operational reality: What management think is going on is often very different from what the workforce believes.
Considering all the published criticism of Zero Harm as a concept, I do not think it is unfair that the onus should be on Zero Harm organisations – including government regulators – to demonstrate that Zero Harm achieves its intended purpose and does not have a negative impact on safety.
Now, this is more than a matter of semantics. Aspirational statements can, and are used against individuals and organisations.
On 21 August 2009 and uncontrolled release of hydrocarbons occurred on the West Atlas drilling rig operating off the North-West coast of Australia. The incident reawakened the Australian Public to the dangers of offshore oil and gas production, leading to a Commission of Inquiry into the event.
During the Commission the aspirational statements of one organisation was used against an individual. The criticism was that a contractor had removed a piece of safety critical hardware, but not replaced it, and had not been directed by the relevant individual to replace it.
There was some discussion about a presentation provided by the organisation, and that resulted in the following exchange.

Q: All right. If the operator could go to page 0004 of this document, that overhead, which is part of the induction training of drilling supervisors, is entitled “Standards”. Do you see that?
A: Yes.
Q: If you could read what is said there, you would agree it captures, if you like, a profound truth?
A: Yes.
Q: Do you agree that that is a truth not simply applicable to drilling supervisors but also applicable to PTT management onshore?
A: Yes.
Q: I want to suggest to you, sir, that your decision not to instruct Mr O’Shea or Mr Wishart to reinstall the 9-5/8″ PCC represents a very significant departure from what is described on that screen.
A: Yes, I can concede that.
Q: Without wishing to labour the point, your decision not to insist upon the reinstallation of the 9-5/8″ PCC was a failure in both leadership and management on your part?
A: Yes, that’s what it seems now.
Q: With respect, sir, I’m suggesting to you that, faced with the circumstances you were, your deference, as it were, to not treading on the toes of the rig personnel and insisting on the reinstallation was, at that point in time, a failure in leadership and management on your part.
A: I will accept that.
How many of these untested platitudes infect organisations, waiting for the opportunity to expose the business to ridicule and criticism?
Or consider if you will, the following scenario. An employee is dismissed for breaching mobile phone requirements when his mobile phone was found in the cabin of the truck he had been operating.
The employee bought an unfair dismissal claim and the presiding tribunal found that there was a valid reason to terminate his employment. However, the tribunal also found that the termination was unfair for several procedural reasons. In part, the tribunal relied on the level of training and information that the employee had been provided about the relevant procedure.
The training documentation provided did not clearly demonstrate that employees were trained in this new procedure and signed accordingly, or that it was given a significant roll-out to employees commensurate with their ‘zero tolerance’ attitude to incidents of breaches, given how this case has been pursued (my emphasis added).
If you are going to have a “Zero” aspiration, that has to be reflected in your business practices. It seldom is.
What I think these examples illustrate is an inherent weakness in the way health and safety is managed. We, as an industry, are overwhelmingly concerned with “how” we manage health and safety risks without paying anything like enough attention to whether the “how” works.
Do all of our aspirations and activities actually manage health and safety risks, or are we just keep keeping people busy or worse, wasting their time? As importantly, how do we know our initiatives are not part of the problem?
BP’s corporate management mandated numerous initiatives that applied to the U.S. refineries and that, while well-intentioned, have  overloaded personnel at BP’s U.S. refineries. This “initiative overload” may have undermined process safety performance at the U.S. refineries. (The Report of the BP US Refineries Independent Safety Review Panel (Baker Panel Review), page xii).
overloaded personnel at BP’s U.S. refineries. This “initiative overload” may have undermined process safety performance at the U.S. refineries. (The Report of the BP US Refineries Independent Safety Review Panel (Baker Panel Review), page xii).
There is no doubt that safety is not the only management discipline that suffers from these deficiencies: “style over substance” and “window dressing”. But if we claim the high moral ground of protecting human health and life, then perhaps the onus on us to show what we do works, is also higher.
On 2 May 2017, I am running a HSE assurance workshop in conjunction with Roy Fitzgerald from Meta-Dymensions.
The program will teach participants the key legal principles for demonstrating effective HSE assurance and how to develop a methodology for demonstrating and evidencing that HSE hazards and risks are being managed as low as reasonably practicable.
As part of the workshop, participants need to bring information about a HSE hazard in their workplace and during the workshop will apply the assurance methodology to:
· Build an assurance process for that hazard; and
· Create a framework to demonstrate and evidence whether (or the extent to which) the hazard is managed as low as reasonably practicable.
Participants will be required to bring information about the hazard and how it is controlled, including policies, procedures, standards and so on. Ideally photographs, diagrams and maps if applicable.
The hazard that participants review should not be too complex. It is more important that participants work through a hazard to ensure they understand and can apply the methodology. Once they have the understanding, they will be able to apply it to more complex hazards.
Spaces in the workshop are limited, and we do not anticipate more than 20 participants for this program. However, to participate, you must send at least two or three participants so they can discuss and work together on reviewing the hazard and developing the assurance processes. You can only send a maximum of three participants.
You can find more information about the workshop, including venues and prices HERE, but please give contact me a call if you have any questions would like to discuss the workshop.
I approach this article with some trepidation.
I was recently sent a copy of Safe Work Australia’s report, Measuring and Reporting on Work Health & Safety, and subsequently saw a post on LinkedIn dealing with the same. I made some observations on the report in response to the original post which drew the ire of some commentators (although I may be overstating it and I apologise in advance if I have), but I did promise a more fulsome response, and in the spirit of a heartfelt desire to contribute to the improvement of health and safety in Australia – here it is.
I want to start by saying, that I have the utmost respect for the authors of the report and nothing is intended to diminish the work they have produced. I also accept that I am writing from a perspective heavily influenced by my engagement with health and safety through the legal process.
I also need to emphasise that I am not dismissing what is said in the report, nor saying that some of the structures and processes proposed by the report are not valid and valuable. But I do think the emphasis in the report on numerical and graphical information has the potential to blind organisations to the effectiveness of crucial systems.
I also want to say that I have witnessed over many years – and many fatalities – organisations that can point to health and safety accreditations, health and safety awards, good personal injury rate data, good audit scores and “traffic lights” all in the green. At the same time, a serious accident or workplace fatalities exposes that the same “good” safety management systems are riddled with systemic failure – long term systemic departures from the requirements of the system that had not been picked up by any of the health and safety measures or performance indicators.
I am not sure how many ways I can express my frustration when executive leadership hold a sincere belief that they have excellent safety management systems in place, only to realise that those systems do not even begin to stand up to the level of scrutiny they come under in a serious legal process.
In my view, there is a clarity to health and safety assurance that has been borne out in every major accident enquiry, a clarity that was overlooked by the drafters of WHS Legislation and a clarity which is all too often overlooked when it comes to developing assurance programs. With the greatest respect, possible to the authors of this report, I fear this has been overlooked again.
In my view, the report perpetuates activity over assurance, and reinforces that assumptions can be drawn from the measure of activity when those assumptions are simply not valid.
Before I expand on these issues, I want to draw attention to another point in the report. At page 38 the report states:
“Each injury represents a breach of the duty to ensure WHS”
To the extent that this comment is meant to represent in some way the “legal” duty, I must take issue with it. There is no duty to prevent all injuries, and injury does not represent, in and of itself, a breach of any duty to “ensure WHS”. The Full Court of the Western Australia Supreme Court made this clear in Laing O’Rourke (BMC) Pty Ltd v Kiwin [2011] WASCA 117 [31], citing with approval the Victorian decision, Holmes v RE Spence & Co Pty Ltd (1992) 5 VIR 119, 123 – 124:
“The Act does not require employers to ensure that accidents never happen. It requires them to take such steps as are practicable to provide and maintain a safe working environment.”
But to return to the main point of this article.
In my view, the objects of health and safety assurance can best be understood from comments of the Pike River Royal Commission:
“The statistical information provided to the board on health and safety comprised mainly personal injury rates and time lost through accidents … The information gave the board some insight but was not much help in assessing the risks of a catastrophic event faced by high hazard industries. … The board appears to have received no information proving the effectiveness of crucial systems such as gas monitoring and ventilation.”
I have written about this recently, and do not want to repeat those observations again (See: Everything is Green: The delusion of health and safety reporting), so let me try and explain this in another way.
Whenever I run obligations training for supervisors and managers we inevitably come to the question of JHAs – and I am assuming that readers will be familiar with that “tool” so will not explain it further.
I then ask a question about how important people think the JHA is. On a scale of 1 to 10, with 1 being the least important and 10 being the most, how important is the JHA?
Inevitably, the group settles on a score of somewhere between 8 and 10. They all agree that the JHA is “critically important” to managing health and safety risk in their business. They all agree that every high hazard activity they undertake requires a JHA.
I then ask, what is the purpose of the JHA. Almost universally groups agree that the purpose of the JHA is something like:
So, my question is, if the JHA is a “crucial system” or “critically important” and a key tool for managing every high-risk hazard in the workplace, is it unreasonable to expect that the organisation would have some overarching view about whether the JHA is achieving its purpose?
They agree it is not unreasonable, but such a view does not exist.
I think the same question could be asked of every other potentially crucial safety management system including contractor safety management, training and competence, supervision, risk assessments and so on. If we look again to the comments in the Pike River Royal Commission, we can see how important these system elements are:
“Ultimately, the worth of a system depends on whether health and safety is taken seriously by everyone throughout an organisation; that it is accorded the attention that the Health and Safety in Employment Act 1992 demands. Problems in relation to risk assessment, incident investigation, information evaluation and reporting, among others, indicate to the commission that health and safety management was not taken seriously enough at Pike.”
But equally, the same question can be asked of high-risk “hazards” – working at heights, fatigue, psychological wellbeing etc.
What is the process to manage the hazard, and does it achieve the purpose it was designed to achieve?
The fact that I have 100% compliance with closing out corrective actions tells me no more about the effectiveness of my crucial systems than the absence of accidents.
The risk of performance measures that are really measures of activity is tha they can create an illusion of safety. The fact that we have 100% compliance with JHA training, a JHA was done every time it was required to be done, or that a supervisor signed off every JHA that was required to be signed off – these are all measures of activity, they do not tell us whether the JHA process has achieved its intended purpose.
So, what might a different type of “assurance” look like?
First, it would make a very conscious decision about the crucial systems or critical risks in the organisation and focus on those. Before I get called out for ignoring everything else, I do not advocate ignoring everything else – by all means, continue to use numerical and similar statistical measures for the bulk of your safety, but when you want to know that something works – you want to prove the effectiveness of your crucial systems – make a conscious decision to focus on them.
I thought that the JHA process was a crucial system, I would want to know how that process was supposed to work? If it is “crucial”, I should understand it to some extent.
I would want a system of reporting that told me whether the process was being managed the way it was supposed to be. And whether it worked. I would like to know, for example:
I would also want to know what triggers were in place to review the quality of the JHA process – was our documented process a good process? Have we ever reviewed it internally? Do we ever get it reviewed externally? Are there any triggers for us to review our process and was it reviewed during the reporting period – if we get alerted to a case where an organisation was prosecuted for failing to implement its JHA process, does that cause us to go and do extra checks of our systems?
We could ask the same questions about our JHA training.
I would want someone to validate the reporting. If I am being told that our JHA process is working well – that it is achieving the purpose it was designed for – I would like someone (from time to time) to validate that. To tell me, “Greg, I have gone and looked at operations and I am comfortable that what you are being told about JHAs is accurate. You can trust that information – and this is why …”.
As part of my personal due dilligence, if I thought JHA were crucial, when I went into the field, that is what I would check too. I would validate the reporting for myself.
I would want some red flags – most importantly, I would want a mandatory term of reference in every investigation requiring the JHA process to be reviewed for every incident – not whether the JHA for the job was a good JHA, but whether our JHA process achieved its purpose in this case, and if not, why not.
If my reporting is telling me that the JHA process is good, but all my incidents are showing that the process did not achieve its intended purpose, then we may have systemic issues that need to be addressed.
I would want to create as many touch points as possible with this crucial system to understand if it was achieving the purpose it was intended to achieve.
My overarching concern, personally and professionally, is to structure processes to ensure that organisations can prove the effectiveness of their crucial systems. I have had to sit in too many little conference rooms, with too many managers who have audits, accreditations, awards and health and safety reports that made them think everything was OK when they have a dead body to deal with.
I appreciate the attraction of traffic lights and graphs. I understand the desire to find statistical and numerical measures to assure safety.
I just do not think they achieve the outcomes we ascribe to them.
They do not prove the effectiveness of crucial systems.
I do not think that there is any serious view suggesting that “leadership” is not an important, if not the most important driver of safety performance. One of the main findings from a 2002 review of Safety Culture was:
… management was the key influence of an organisation’s safety culture. A review of the safety climate literature revealed that employees’ perceptions of management’s attitudes and behaviours towards safety, production and issues such as planning, discipline etc. was the most useful measurement of an organisation’s safety climate. The research indicated that different levels of management may influence health and safety in different ways, for example managers through communication and supervisors by how fairly they interact with workers (Thompson, 1998). Thus, the key area for any intervention of an organisation’s health and safety policy should be management’s commitment and actions towards safety (Safety Culture: A review of the literature).
In the wake of findings like these, and numerous others, it is unsurprising that safety leadership often dominates discussions about safety management.
But are there conversations about safety leadership that we are not having and should be?
To my mind, the hard work in health and safety management is understanding if, or the extent to which, health and safety risks in our business are being controlled. All too often, however, in my experience “leadership” is an excuse to avoid the hard work of health and safety management.
The “psychology” (and I use that term as a complete layperson) of safety leadership seems to be that if I can convince my workforce that I genuinely care for them and that safety is genuinely important, then safety will take care of itself.
If I “care“, if I am a “safety leader” I do not need to do the hard work to critically challenge incident investigations, I do not need to analyse, understand and challenge audits. If I am a “safety leader” then I can accept declining personal injury rates and green traffic lights on my corporate scorecard as evidence that my safety management system is working, without ever having to challenge the assumptions that underpinned that information. Assumptions that have been shown time and again to be wrong.
This is the same discourse that threaded its way through safety culture: It doesn’t matter how bad our management systems are because we have a good “culture“. It is also the same discourse that is starting to creep into the next wave of safety thinking, concepts like “safety differently” and “appreciative enquiry“.
I make no comment on the efficacy of leadership, culture, safety differently, appreciative enquiry or whatever the next trend will be but I do question where, in any of these concepts, we do the hard work of confirming that our risks are being controlled.
I recall many years ago reviewing a matter where a worker sent a hazardous substance through the internal mail using a yellow into office envelope (back when they existed). The worker broke every one of the organisations procedures and protocols for managing hazardous substances, yet the organisation viewed this dangerous event as a triumph of their “culture“, because the worker “cared“.
The twisted logic where organisations use leadership or culture to wallpaper over the cracks of ineffective safety management systems, and actively avoid the hard work of understanding if their risks are being controlled, is very often bought into stark relief following a disaster.
The next time you are in a meeting discussing safety management listen to see if leadership or culture is being used as an avoidance strategy. Are the difficult topics such as improving the quality of incident investigation or clarifying complex and bureaucratic safety management systems or improving risk assessments bypassed with comments like:
we just need to get out and be seen more
or
we just need to spend more time in the field talking to the blokes
Is this leadership or an excuse to avoid the hard work?
Over and above avoiding what really needs to be done, is it possible that the things we do in the name of “leadership” have the potential to actively undermine safety in our organisations?
Whatever your “leadership” objective might be, whether it is to demonstrate commitment, to understand the work being performed in your organisation, to appreciate what might be preventing people from complying with safety procedures or any other objective, how do you know that your actions in the name of leadership are achieving those objectives? Because for all your good intentions there is a real risk that your presence in the field talking about safety might have the opposite effect. It might promote cynicism amongst your workforce, it might disengage them from your safety message.
You may be seen as a leader whose only concern is to cover their own backside and who obsesses over safety issues important to you, without really listening to the concerns of the workforce.
How do you know if your safety leadership works?
I think that much of what is done in the name of safety and health has, consciously or unconsciously, devolved into “window dressing“. Much of what we do is held up to the public or to our workforce as evidence of our commitment to safety, yet the substantive hard work necessary to understand if our health and safety risks are being managed remains undone – the façade of health and safety management is attractive but the building is crumbling.
Safety leadership and related concepts of care and culture have a place. More than that, they are critically important. But they are not buzzwords to be lightly tossed around and as a critical process, leadership deserves the same level of scrutiny and analysis as any of your other critical processes.
In August 2016, I wrote a WHS Update about the High Court decision, Deal v Father Pius Kodakkathanath [2016] HCA 31 which considered the legal test of Reasonably Practicable in the context of Australian health and safety legislation. Shortly after that, one of my connections on Linkedin posted an article about Reasonably Practicable. The article offered an engineering perspective on “As Low as Reasonably Practicable” (ALARP), stating:
… recent developments in Australian workplace health and safety law place proactive responsibilities on senior personnel in organisations, so they must be fully informed to make proper decisions
This sentiment seemed similar to an earlier engineering publication which argued that ALARP and “So Far as is Reasonably Practicable” (SFARP) were different and that this difference was, in part a least as result of “harmonised”, WHS legislation.
In both cases, I believed the articles were misaligned with the legal construct of Reasonably Practicable and misrepresented that there had been a change in the legal test of Reasonably Practicable prompted by changes to WHS legislation.
This background caused me to reflect again on the notion of Reasonably Practicable and what it means in the context of legal obligations for health and safety.
To start, I do take issue with the suggestion that changes to WHS legislation have resulted in a shift in what Reasonably Practicable means. The basis of this idea seems to be an apparent change in terminology from ALARP to SFARP.
The term SFARP was in place in health and safety legislation before the introduction of WHS and jurisdictions that have not adopted WHS legislation still use the term. For example, the primary obligations under the Victorian Occupational Health and Safety Act 2004 are set out in section 20, and state:
To avoid doubt, a duty imposed on a person by this Part or the regulations to ensure, so far as is reasonably practicable, health and safety requires the person …
Indeed, the architects of WHS legislation[1] specifically retained the term Reasonably Practicable because it was a common and well-understood term in the context of Australian health and safety legislation:
5.51 Reasonably practicable is currently defined or explained in a number of jurisdictions. The definitions are generally consistent, with some containing more matters to be considered than others. The definitions ‘are consistent with the long settled interpretation by courts, ‘in Australia and elsewhere.
5.52 The provision of the Vic Act relating to reasonably practicable was often referred to in submissions (including those of governments) and consultations as either a preferred approach or a basis for a definition of reasonably practicable.
5.53 We recommend that a definition or section explaining the application of reasonably practicable be modelled on the Victorian provision. We consider that, with some modification, it most closely conforms to what would be suitable for the model Act. [My emphasis added]
In my view, it is unarguable that the concept of Reasonably Practicable has been well-settled in Australian law for a considerable period, and the concept has not changed with the introduction of WHS legislation.
If we accept that Reasonably Practicable has been consistently applied in Australia for some time, the next question is, what does it mean?
Reasonably Practicable is a defined term in most health and safety legislation in Australia. Section 20(2) of the Victorian Occupational Health and Safety Act 2004, for example, states:
(2) To avoid doubt, for the purposes of this Part and the regulations, regard must be had to the following matters in determining what is (or was at a particular time) reasonably practicable in relation to ensuring health and safety—
(a) the likelihood of the hazard or risk concerned eventuating;
(b) the degree of harm that would result if the hazard or risk eventuated;
(c) what the person concerned knows, or ought reasonably to know, about the hazard or risk and any ways of eliminating or reducing the hazard or risk;
(d) the availability and suitability of ways to eliminate or reduce the hazard or risk;
(e) the cost of eliminating or reducing the hazard or risk.
In the High Court decision, Slivak v Lurgi (Australia) Pty Ltd [2001] HCA 6, Justice Gaudron described Reasonably Practicable as follows:
The words “reasonably practicable” have, somewhat surprisingly, been the subject of much judicial consideration. It is surprising because the words “reasonably practicable” are ordinary words bearing their ordinary meaning. And the question whether a measure is or is not reasonably practicable is one which requires no more than the making of a value judgment in the light of all the facts. Nevertheless, three general propositions are to be discerned from the decided cases:
Another High Court decision, Baiada Poultry Pty Ltd v The Queen [2012] HCA 14, emphasised similar ideas.
The case concerned that the death of a subcontracted worker during forklift operations. Baiada was the Principal who had engaged the various contractors to perform the operations and in an earlier decision the court had concluded:
it was entirely practicable for [Baiada] to required contractors to put loading and unloading safety measures in place and to check whether those safety managers were being observed from time to time ((2011) 203 IR 396 at 410)
On appeal, the High Court framed this finding differently. They observed:
As the reasons of the majority in the Court of Appeal reveal by their reference to Baiada checking compliance with directions it gave to [the contractors], the question presented by the statutory duty “so far as is reasonably practicable” to provide and maintain a safe working environment could not be determined by reference only to Baiada having a legal right to issue instructions to its subcontractors. Showing that Baiada had the legal right to issue instructions showed only that it was possible for Baiada to take that step. It did not show that this was a step that was reasonably practicable to achieve the relevant result of providing and maintaining a safe working environment. That question required consideration not only of what steps Baiada could have taken to secure compliance but also, and critically, whether Baiada’s obligation “so far as is reasonably practicable” to provide and maintain a safe working environment obliged it: (a) to give safety instructions to its (apparently skilled and experienced) subcontractors; (b) to check whether its instructions were followed; (c) to take some step to require compliance with its instructions; or (d) to do some combination of these things or even something altogether different. These were questions which the jury would have had to decide in light of all of the evidence that had been given at trial about how the work of catching, caging, loading and transporting the chickens was done.[3] [my emphasis added]
In light of these, and other decided cases it is possible to form a practical test to consider what is Reasonably Practicable. In my view, it is necessary for an organisation to demonstrate that they:
What constitutes Proper Systems and Adequate Supervision is a judgement call that needs to be determined with regard to the risks. It requires an organisation to balance the risk against the cost, time and trouble of managing it.[4]
It is also worth noting at this point, that Reasonably Practicable is, generally speaking, an organisational obligation. It is not an individual,[5] and in particular, it is not an employee obligation.
I often see, when working with clients, safety documents required be signed by employees that the state that risks have been controlled to “ALARP”. This is not the employee’s responsibility and the extent to which an employee does or does not control the risk to ALARP does not affect an employer’s obligations.
In broad terms, it is the organisation’s (PCBU or employer) obligation to manage risks as low as, or so far as is, Reasonably Practicable. The employee obligation is to do everything “reasonable”. This includes complying with the organisation’s systems.
It is the organisation’s obligation to identify the relevant health and safety risks and define how they will be controlled, ensuring that the level of control is “Reasonably Practicable. It is the employee’s obligation to comply with the organisation’s requirements.
So, what might Reasonably Practicable look like in practice?
I recently defended a case that involved a worker who was seriously injured at work. Although the injury did not result from a fall from height, the prosecution case against my client was based on failure to meet its obligations about working at heights.
My client had, on any measure, a Proper System for managing the risk of work at heights. They had a documented working at height Standard and Procedure both of which were consistent with industry best practice and regulator guidance material. All work at height above 1.8 m required a permit to work and a JHA. The documented procedures prescribed appropriate levels of supervision and training.
In the three years before the relevant incident, my client had not had a working at height incident of any sort nor had they had a health and safety incident at all. Based on all of our investigations as part of preparing the case, there was nothing to suggest that the incident information was not legitimate.
The activity which was being performed at the time of the incident was conducted routinely, at least weekly, at the workplace.
In looking to construct a Reasonably Practicable argument to defend the case what would we be trying to do? In essence, I would be trying to establish that the incident was an aberration, a “one off departure” from an otherwise well understood, consistently applied system of work that was wholly appropriate to manage the risk of working at heights.
In practice, that would mean:
There may be other information that we would seek, but in broad terms, the information outlined above helps to build a case that there was a proper system that was effectively implemented and that:
What happened?
Rather than be able to demonstrate that the incident was a one-off departure from an otherwise effective system, the evidence revealed a complete systemic failure. While the documented system was a Proper System and complied with all relevant industry standards and guidelines, it was not implemented in practice.
Most compelling was the fact that, despite this being a weekly task, there was not a single instance of the working at height Standard and Procedure been complied with. We could not produce a single example where either the injured worker or indeed any worker who had performed the task had done so under an approved permit to work with an authorised JHA.
All of the workers gave evidence that the primary risk control tool on site was a Take 5. The Take 5 is a preliminary risk assessment tool, and only if that risk assessment scored 22 or above was a JHA required. The task in question was always assessed as 21. The requirement for a JHA, in the minds of the workforce, was never triggered and none of them understood the requirements of the Standard or Procedure.
To me, this case is entirely indicative of the fundamental failure of Reasonably Practicable in most workplaces. In the vast majority of cases that I have been involved in the last 25 years, organisations have systems that would classify as Proper Systems. They are appropriate to manage the risk that they were designed to manage.
Equally, organisations cannot demonstrate Adequate Supervision. While there may be audits, inspections, checking and checklists – there is no targeted process specifically designed to test and understand whether the systems in place to manage health and safety risks in the business are in fact implemented and are effective to manage those risks.
In my experience, most organisations spend far too much time trying to devise the “perfect” Proper System. We spend far too little time understanding what needs to be done to confirm that the System works, and then leading the confirmation process.
Reasonably Practicable has not changed.
Reasonably Practicable is not a numeric equation.
Reasonably Practicable changes over time.
Reasonably Practicable is an intellectual exercise and a judgement call to decide how an organisation will manage the health and safety risks in its business.
Reasonably Practicable requires an organisation to demonstrate that they:
What constitutes Proper Systems and Adequate Supervision is a judgement call that needs to be determined with regard to the risks. It requires an organisation to balance the risk against the cost, time and trouble of managing it.
[1] See the National Review into Model Occupational Health and Safety Laws: First Report, October 2008.
[2] Slivak v Lurgi (Australia) Pty Ltd [2001] HCA 6 [53].
[3] Baiada Poultry Pty Ltd v The Queen [2012] HCA 14 [33].
[4] See also: Safe Work NSW v Wollongong Glass P/L [2016] NSWDC 58 and Collins v State Rail Authority of New South Wales (1986) 5 NSWLR 209.
[5] There are some exceptions to this where an individual, usually a manager or statutory officeholder will be required to undertake some action that is Reasonably Practicable.
This article is a general discussion about Reasonably Practicable and related concepts. it should not be relied on, and is not intended to be specific legal advice.
There has been some discussions and commentary in various online forums recently looking at the issue of “positive” incident investigations. Although there seems to be a variety of nuances in the description of positive investigations they focus on “what went right“.
Some of these investigation models have also incorporated a broader management technique of “appreciative enquiry“, which, as I understand it, came to prominence in the late 1980’s (see HERE for examples and information about appreciative enquiry).
The discussion about these frameworks describes the “what went right” philosophy as a positive view of investigations. It is a philosophy that does not focus on blame, but promotes discussion:
The benefit of that approach is that the conversation with witnesses is an entirely positive one. It is not about what could have happened. Not about the doom and gloom narrowly averted. Rather, it is about their heroic act, well designed process or lucky event that allowed us to avoid the adverse outcome. People love talking about positive things particularly if they had something to do with them. (https://www.linkedin.com/pulse/investigate-your-serious-near-misses-positive-way-michael-tooma?trk=prof-post)
In my view, when organisations are not mature enough to talk about issues in a non-judgmental way, without attribution of blame, the “what went right” enquiry may present a risk. It may be seen as a contrivance, with the facilitator spending a lot of their time saying things like “remember this is not about blame“.
In “mature” organisations the need to construct a system of enquiry to focus on the positive and avoid discussion of blame is largely redundant because the participants are aligned with and support the goals of the organisation. Their desire to support the goals of the organisation overrides any petty, personal concerns about individual praise or blame.
If you have ever been privileged enough to work with high-performance sporting teams or elite military forces, you will understand this idea.
A precondition of belonging to these groups is the willingness to say and hear things that support the group’s objectives without personal agendas or taking personal affront. The newest member of the team has a license to speak frankly about the performance of the most senior, and the most senior is expected to accept that conversation, not in the context of them personally, but in the context of the overall objectives of the team.
The extent to which organisations have to contrive a system whereby participants are corralled by a “what went right” narrative says a lot about the culture of an organisation and the “buy in” that people have to team objectives.
That is not to say that appreciative enquiry or investigating “what went right” does not have a place in organisations, nor that it could be an important building block along the way to developing something like an elite performing team. But as a word of caution, you should also understand some of the paradoxes involved.
The Safety Paradox supposes that any initiative done in the name of health and safety has the potential to both improve and damage health and safety in a workplace.
Having sat through appreciative enquiry “management brainstorming sessions” and incident investigations there is a strong sense of “flavour of the month” initiative as well as an even stronger sense of avoiding accountability. An overriding impression of a process delivered without context or explanation – why this and why now? The end product is a wall of butcher’s paper populated with sweeping motherhood statements and management speak, completely absent any meaningful desire to manage known problems.
The pendulum, it seemed, had swung too far the other way.
Again, that is not to say it is not an idea that should not be explored and applied. But it needs context. It needs explanation; it needs skilful facilitation, and it needs, perhaps most importantly, dedicated and meaningful follow-up with implementation. Otherwise? Well, we have all been in “those” types of sessions.
Another aspect of the “what went right” investigations is the requirement for something to have occurred. There needs to be an incident or near miss to trigger the enquiry.
A risk in the “what went right” enquiry (without more) is that it can contribute to the illusion of safety.
The illusion of safety is the gap between safety management as we imagine it in our organisation and what happens in practice. Incident investigations can be a powerful tool in exposing the illusion of safety because they have the potential to illustrate the disconnect between what we think happens and what is happening. By just focusing on “what went right“, particularly in near miss incidents, we may fuel the illusion of safety and create a narrative that our systems are working to protect us from these incidents – effectively papering over the cracks in the edifice.
While avoiding blame and promoting open discussion is important, so too is avoiding sugar-coating the situation. Again, balance, transparency and genuine enquiry ought to be the goal.
I would like to suggest something different – investigating work as it is performed; investigating when nothing happens.
An investigation framework that I find useful uses systems as opposed to causal analysis.
It supposes that organisations have systems and processes in place to prevent certain things from happening and tries to understand:
From there, we identify and try to explain the “gap” between what should have happened and what did happen.
This framework is not concerned with “causation“. All identified gaps are given equal attention and analysis, regardless of their potential causal relationship with the incident. They are all important because they all represent a potential systemic weakness in safety management which, given a different factual matrix, could be causal.
The attractiveness of this framework is that it can help you identify systemic weakness when nothing has happened.
A few years ago I was involved in an incident leading to the prosecution of a client following a working at heights incident. The incident and the various investigations that followed revealed the usual list of suspects:
As part of working with that client, we applied the systems analysis framework to a range of other, similar high-risk work, including:
In every case, the work had been performed “successfully“, without incident or near miss.
However, the analysis of the gap between how the work should have been performed and how it was performed demonstrated the same types of “failures” in the way that work was ordinarily performed as when the incident occurred.
In other words, even when work was “successful”, procedures were not followed, risks were not identified as well as they could have been, training was not complied with, documentation was not completed and so on.
The systemic weaknesses were not just present at the time of the incident. They were characteristic of the way work was performed in the days and months previously.
The incident was not a one-off departure from an otherwise “good” system – it was simply evidence of otherwise broader, systemic failures.
Moreover, this system analysis approach highlighted weaknesses hidden by the traditional safety metrics – injury rates, action items closed out, hazards reported, management site visits, etc. – all of which were “green“.
I have applied this method of review from time to time over the years where I have been able to convince clients of its value. On every occasion it brings to light the gap between the safety as imagined and safety in practice, lifting the veil on the illusion of safety.
In the Pike River Royal Commission, the Commission carefully examined Pike River’s system of incident investigation to understand if it “worked“. They reviewed 1083 incident investigations and did a detailed examination of 436 of them. Managers were subject to examination of their understanding of the investigation process, and ultimately the Commission found that “incidents were never properly investigated“.
You can see an example of the examination of management HERE.
Weakness in incident investigations, amongst other important systems elements, formed the basis of significant criticism of Pike River and its management:
Ultimately, the worth of a system depends on whether health and safety is taken seriously by everyone throughout an organisation; that it is accorded the attention that the Health and Safety in Employment Act 1992 demands. Problems in relation to risk assessment, incident investigation, information evaluation and reporting, among others, indicate to the commission that the health and safety management was not taken seriously enough at Pike.
What do your philosophy and implementation of incident investigations say about you?


